The UNMC dermatopathology service is headed by Dominick DiMaio, MD and includes specialist, Scott R. Lauer, MD A wide range of services are available for the examination of dermatopathology specimens received at the UNMC, including a wide panel of immunoperoxidase stains, direct immunofluorescence staining, fluorescence in situ hybridization staining and molecular studies to determine the presence of either T cell or B cell clonal populations in the evaluation of cutaneous lymphomas. In 2017, a total of 10,578 dermatopathology specimens were reviewed of which 1,209 represented outside slide consultations and 337 direct immunofluorescence specimens.
Any questions regarding dermatopathology specimens can be directed to Dr. DiMaio at 402-559-4186.
Below is an example of the thousands of specimens seen by our dermatopathologists.
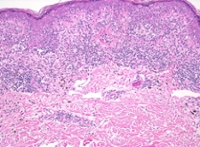
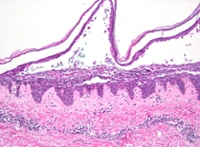 IgG/IgA pemphigus: IgG/IgA pemphigus:The biopsy demonstrates the presence of a suprabasilar blister associated with neutrophilic inflammation suggestive of pemphigus vulgaris. Subsequent direct immunofluorescence staining, however, showed intercellular for both IgG and IgA which makes the diagnosis most consistent with IgG/IgA pemphigus. |
|
|
|
|
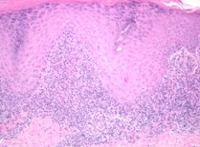
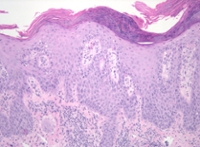
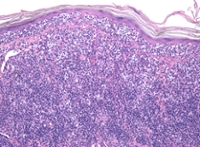
 Melanoma: Melanoma:The biopsy demonstrates nests and individual melanocytes along the dermal epidermal junction. There is confluent and pagetoid spread of cytologically atypical individual melanocytes. Within the dermis there are occasional individual melanocytes associated with a brisk inflammatory host response. These features are consistent with invasive melanoma. |
|
|
|
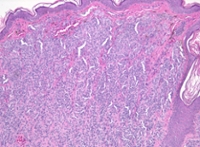
Pagetoid Reticulosis: |